Pes Planus Explained
Overview

Flat feet indicates that no arch is present and the underside of the foot lies completely flat on the ground. The true 'flat foot' is very rare. In fact, less than 5% of the population have flat feet with no arch present whatsoever. It is quite normal for small children to have flat feet, however the arch usually develops as they get older. If the arch hasn't developed yet by the age of 5 or 6 the child may need children's orthotics.
Causes
Over-pronation is a common biomechanical problem that occurs when the arches collapse while walking or standing. This condition hampers our natural walking pattern, causing an imbalance, and leading to wear and tear in other parts of the body with every step we take. Whether you suffer from over-pronation like most of the population, or you have a true flat foot, in both cases your poor walking pattern may contribute to a range of different complaints. As we age, poor aligment of the feet causes very common conditions such as heel pain or knee pain. Over-pronation has different causes. Obesity, pregnancy, age or repetitive pounding on a hard surface can weaken the arch, leading to over-pronation. Over-pronation is also very common with athletes, especially runners, who most of them nowadays use orthotics inside their shoes.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
Your doctor will ask about your symptoms and medical history. A physical and foot exam will be done. Flat feet can be diagnosed by appearance. To determine if the foot is rigid, you may be asked to do some simple tasks.
What does it mean when you have flat feet?
Non Surgical Treatment
In many cases of PTTD, treatment can begin with non-surgical approaches that may include orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support.
Surgical Treatment

Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated.
Flat feet indicates that no arch is present and the underside of the foot lies completely flat on the ground. The true 'flat foot' is very rare. In fact, less than 5% of the population have flat feet with no arch present whatsoever. It is quite normal for small children to have flat feet, however the arch usually develops as they get older. If the arch hasn't developed yet by the age of 5 or 6 the child may need children's orthotics.
Causes
Over-pronation is a common biomechanical problem that occurs when the arches collapse while walking or standing. This condition hampers our natural walking pattern, causing an imbalance, and leading to wear and tear in other parts of the body with every step we take. Whether you suffer from over-pronation like most of the population, or you have a true flat foot, in both cases your poor walking pattern may contribute to a range of different complaints. As we age, poor aligment of the feet causes very common conditions such as heel pain or knee pain. Over-pronation has different causes. Obesity, pregnancy, age or repetitive pounding on a hard surface can weaken the arch, leading to over-pronation. Over-pronation is also very common with athletes, especially runners, who most of them nowadays use orthotics inside their shoes.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
Your doctor will ask about your symptoms and medical history. A physical and foot exam will be done. Flat feet can be diagnosed by appearance. To determine if the foot is rigid, you may be asked to do some simple tasks.
What does it mean when you have flat feet?
Non Surgical Treatment
In many cases of PTTD, treatment can begin with non-surgical approaches that may include orthotic devices or bracing. To give your arch the support it needs, your foot and ankle surgeon may provide you with an ankle brace or a custom orthotic device that fits into the shoe. Immobilization. Sometimes a short-leg cast or boot is worn to immobilize the foot and allow the tendon to heal, or you may need to completely avoid all weight-bearing for a while. Physical therapy. Ultrasound therapy and exercises may help rehabilitate the tendon and muscle following immobilization. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Shoe modifications. Your foot and ankle surgeon may advise changes to make with your shoes and may provide special inserts designed to improve arch support.
Surgical Treatment
Common indications for surgery are cerebral palsy with an equinovalgus foot, to prevent progression and breakdown of the midfoot. Rigid and painful Pes Planus. To prevent progression, eg with a Charcot joint. Tibialis posterior dysfunction, where non-surgical treatment is unsuccessful. Possible surgical procedures include Achilles tendon lengthening. Calcaneal osteotomy, to re-align the hindfoot. Reconstruction of the tibialis posterior tendon. For severe midfoot collapse of the arch, triple arthrodesis may be indicated.
Exercise Movements For Leg Length Discrepancy Following A Broken Femur
Overview
There are generally two kinds of leg length discrepancies. Structural discrepancy occurs when either the thigh (femur) or shin (tibia) bone in one leg is actually shorter than the corresponding bone in the other leg. Functional discrepancy occurs when the leg lengths are equal, but symmetry is altered somewhere above the leg, which in turn disrupts the symmetry of the legs. For example, developmental dislocation of the hip (DDH) can cause a functional discrepancy. In DDH, the top of the leg bone (femur) that is not properly positioned in the hip socket may hang lower than the femur on the other side, giving the appearance and symptoms of a leg length discrepancy.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
The effects vary from patient to patient, depending on the cause of the discrepancy and the magnitude of the difference. Differences of 3 1/2 to 4 percent of the total length of the lower extremity (4 cm or 1 2/3 inches in an average adult), including the thigh, lower leg and foot, may cause noticeable abnormalities while walking and require more effort to walk. Differences between the lengths of the upper extremities cause few problems unless the difference is so great that it becomes difficult to hold objects or perform chores with both hands. You and your physician can decide what is right for you after discussing the causes, treatment options and risks and benefits of limb lengthening, including no treatment at all. Although an LLD may be detected on a screening examination for curvature of the spine (scoliosis), LLD does not cause scoliosis. There is controversy about the effect of LLD on the spine. Some studies indicate that people with an LLD have a greater incidence of low back pain and an increased susceptibility to injuries, but other studies refute this relationship.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Treatments for limb-length discrepancies and differences vary, depending on the cause and severity of the condition. At Gillette, our orthopedic surgeons are experts in typical and atypical growth and development. Our expertise lets us plan treatments that offer a lifetime of benefits. Treatments might include monitoring growth and development, providing noninvasive treatments or therapy, and providing a combination of orthopedic surgical procedures. To date, alternative treatments (such as chiropractic care or physical therapy) have not measurably altered the progression of or improved limb-length conditions. However, children often have physical or occupational therapy to address related conditions, such as muscle weakness or inflexibility, or to speed recovery following a surgical procedure. In cases where surgical treatment isn?t necessary, our orthopedists may monitor patients and plan noninvasive treatments, such as, occupational therapy, orthoses (braces) and shoe inserts, physical therapy, prostheses (artificial limbs).

leg length discrepancy exercises
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
There are generally two kinds of leg length discrepancies. Structural discrepancy occurs when either the thigh (femur) or shin (tibia) bone in one leg is actually shorter than the corresponding bone in the other leg. Functional discrepancy occurs when the leg lengths are equal, but symmetry is altered somewhere above the leg, which in turn disrupts the symmetry of the legs. For example, developmental dislocation of the hip (DDH) can cause a functional discrepancy. In DDH, the top of the leg bone (femur) that is not properly positioned in the hip socket may hang lower than the femur on the other side, giving the appearance and symptoms of a leg length discrepancy.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
The effects vary from patient to patient, depending on the cause of the discrepancy and the magnitude of the difference. Differences of 3 1/2 to 4 percent of the total length of the lower extremity (4 cm or 1 2/3 inches in an average adult), including the thigh, lower leg and foot, may cause noticeable abnormalities while walking and require more effort to walk. Differences between the lengths of the upper extremities cause few problems unless the difference is so great that it becomes difficult to hold objects or perform chores with both hands. You and your physician can decide what is right for you after discussing the causes, treatment options and risks and benefits of limb lengthening, including no treatment at all. Although an LLD may be detected on a screening examination for curvature of the spine (scoliosis), LLD does not cause scoliosis. There is controversy about the effect of LLD on the spine. Some studies indicate that people with an LLD have a greater incidence of low back pain and an increased susceptibility to injuries, but other studies refute this relationship.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Treatments for limb-length discrepancies and differences vary, depending on the cause and severity of the condition. At Gillette, our orthopedic surgeons are experts in typical and atypical growth and development. Our expertise lets us plan treatments that offer a lifetime of benefits. Treatments might include monitoring growth and development, providing noninvasive treatments or therapy, and providing a combination of orthopedic surgical procedures. To date, alternative treatments (such as chiropractic care or physical therapy) have not measurably altered the progression of or improved limb-length conditions. However, children often have physical or occupational therapy to address related conditions, such as muscle weakness or inflexibility, or to speed recovery following a surgical procedure. In cases where surgical treatment isn?t necessary, our orthopedists may monitor patients and plan noninvasive treatments, such as, occupational therapy, orthoses (braces) and shoe inserts, physical therapy, prostheses (artificial limbs).
leg length discrepancy exercises
Surgical Treatment
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.
Heel Pain
Overview
Every mile you walk puts tons of stress on each foot. Your feet can handle a heavy load, but too much stress pushes them over their limits. When you pound your feet on hard surfaces playing sports or wear shoes that irritate sensitive tissues, you may develop heel pain, the most common problem affecting the foot and ankle. A sore heel will usually get better on its own without surgery if you give it enough rest. However, many people ignore the early signs of heel pain and keep on doing the activities that caused it. When you continue to walk on a sore heel, it will only get worse and could become a chronic condition leading to more problems.
Causes
Common causes of heel pain include Achilles tendinitis, Achilles tendon rupture, Bone tumor, Bursitis, Fibromyalgia, Fracture, Gout, Heel pad wear and tear, Heel spur, Osteomyelitis, Peripheral neuropathy, Pinched nerve, Plantar fasciitis, Rheumatoid arthritis, Stress fractures, Tarsal tunnel syndrome, Tendinitis. Causes shown here are commonly associated with this symptom. Work with your doctor or other health care professional for an accurate diagnosis.
Symptoms
Depending on the specific form of heel pain, symptoms may vary. Pain stemming from plantar fasciitis or heel spurs is particularly acute following periods of rest, whether it is after getting out of bed in the morning, or getting up after a long period of sitting. In many cases, pain subsides during activity as injured tissue adjusts to damage, but can return again with prolonged activity or when excessive pressure is applied to the affected area. Extended periods of activity and/or strain of the foot can increase pain and inflammation in the foot. In addition to pain, heel conditions can also generate swelling, bruising, and redness. The foot may also be hot to the touch, experience tingling, or numbness depending on the condition.
Diagnosis
Your doctor will listen to your complaints about your heel and examine you to see what is causing the pain, and whether anything else has started it off. If the cause of your pain seems obvious, your doctor may be happy to start treatment straight away. However, some tests may be helpful in ruling out other problems. Blood tests may be done for arthritis. An Xray will show any arthritis in the ankle or subtalar joint, as well as any fracture or cyst in the calcaneum. (It will also show a spur if you have one, but as we know this is not the cause of the pain.) Occasionally a scan may be used to help spot arthritis or a stress fracture.
Non Surgical Treatment
Home care, in cases that are not severe, home care is probably enough to get rid of heel pain. Rest, avoid running or standing for long periods, or walking on hard surfaces. Avoid activities that may stress the heels. Ice, place an ice-pack on the affected area for about 15 minutes. Do not place bare ice directly onto skin. Footwear. proper-fitting shoes that provide good support are crucial. Athletes should be particularly fussy about the shoes they use when practicing or competing - sports shoes need to be replaced at specific intervals (ask your trainer). Foot supports, wedges and heel cups can help relieve symptoms.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
what does a heel spur look like
Prevention

You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve.
Every mile you walk puts tons of stress on each foot. Your feet can handle a heavy load, but too much stress pushes them over their limits. When you pound your feet on hard surfaces playing sports or wear shoes that irritate sensitive tissues, you may develop heel pain, the most common problem affecting the foot and ankle. A sore heel will usually get better on its own without surgery if you give it enough rest. However, many people ignore the early signs of heel pain and keep on doing the activities that caused it. When you continue to walk on a sore heel, it will only get worse and could become a chronic condition leading to more problems.
Causes
Common causes of heel pain include Achilles tendinitis, Achilles tendon rupture, Bone tumor, Bursitis, Fibromyalgia, Fracture, Gout, Heel pad wear and tear, Heel spur, Osteomyelitis, Peripheral neuropathy, Pinched nerve, Plantar fasciitis, Rheumatoid arthritis, Stress fractures, Tarsal tunnel syndrome, Tendinitis. Causes shown here are commonly associated with this symptom. Work with your doctor or other health care professional for an accurate diagnosis.
Symptoms
Depending on the specific form of heel pain, symptoms may vary. Pain stemming from plantar fasciitis or heel spurs is particularly acute following periods of rest, whether it is after getting out of bed in the morning, or getting up after a long period of sitting. In many cases, pain subsides during activity as injured tissue adjusts to damage, but can return again with prolonged activity or when excessive pressure is applied to the affected area. Extended periods of activity and/or strain of the foot can increase pain and inflammation in the foot. In addition to pain, heel conditions can also generate swelling, bruising, and redness. The foot may also be hot to the touch, experience tingling, or numbness depending on the condition.
Diagnosis
Your doctor will listen to your complaints about your heel and examine you to see what is causing the pain, and whether anything else has started it off. If the cause of your pain seems obvious, your doctor may be happy to start treatment straight away. However, some tests may be helpful in ruling out other problems. Blood tests may be done for arthritis. An Xray will show any arthritis in the ankle or subtalar joint, as well as any fracture or cyst in the calcaneum. (It will also show a spur if you have one, but as we know this is not the cause of the pain.) Occasionally a scan may be used to help spot arthritis or a stress fracture.
Non Surgical Treatment
Home care, in cases that are not severe, home care is probably enough to get rid of heel pain. Rest, avoid running or standing for long periods, or walking on hard surfaces. Avoid activities that may stress the heels. Ice, place an ice-pack on the affected area for about 15 minutes. Do not place bare ice directly onto skin. Footwear. proper-fitting shoes that provide good support are crucial. Athletes should be particularly fussy about the shoes they use when practicing or competing - sports shoes need to be replaced at specific intervals (ask your trainer). Foot supports, wedges and heel cups can help relieve symptoms.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
what does a heel spur look like
Prevention
You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve.
Diagnosing Mortons Neuroma
Overview
 Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men.
Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men.
Causes
Some say that this condition should not be called Morton's neuroma as, in fact, it is not actually a neuroma. A neuroma is a non-cancerous (benign) tumour that grows from the fibrous coverings of a nerve. There is no tumour formation in Morton's neuroma. The anatomy of the bones of the foot is also thought to contribute to the development of Morton's neuroma. For example, the space between the long bones (metatarsals) in the foot is narrower between the second and third, and between the third and fourth metatarsals. This means that the nerves that run between these metatarsals are more likely to be compressed and irritated. Wearing narrow shoes can make this compression worse.
Symptoms
The most common symptom of Morton's neuroma is localized pain in the interspace between the third and fourth toes. It can be sharp or dull, and is worsened by wearing shoes and by walking. Pain usually is less severe when the foot is not bearing weight.
Diagnosis
During the exam, your doctor will press on your foot to feel for a mass or tender spot. There may also be a feeling of "clicking" between the bones of your foot. Some imaging tests are more useful than others in the diagnosis of Morton's neuroma. Your doctor is likely to order X-rays of your foot, to rule out other causes of your pain such as a stress fracture. Ultrasound. This technology uses sound waves to create real-time images of internal structures. Ultrasound is particularly good at revealing soft tissue abnormalities, such as neuromas. Magnetic resonance imaging (MRI). Using radio waves and a strong magnetic field, an MRI also is good at visualizing soft tissues. But it's an expensive test and often indicates neuromas in people who have no symptoms.
Non Surgical Treatment
Depending on your overall health, symptoms and severity of the neuroma, the condition may be treated conservatively and/or with surgery. Non-surgical methods for neuroma are aimed at decreasing and/or eliminating symptoms (pain). Wear proper supportive shoes. Use an arch support. Wear shoes with a wide toe box. Modify your activities. Lose weight. Wear shoes with cushion. Prescribe an oral anti-inflammatory medication. Anti-inflammatory medication is useful to significantly reduce pain and inflammation. A physical therapist may perform ultrasound and other techniques to reduce inflammation. You will also be instructed how to stretch your foot and leg properly. Padding and/or cushioning of the ball of the foot is an effective method of preventing physical irritation with shoes. A custom foot orthotic is a doctor prescribed arch support that is made directly from a casting (mold) of your feet, and theoretically should provide superior support compared to shoe insert that you would purchase from a pharmacy. A cortisone injection is a powerful anti-inflammatory medication that is used to rapidly reduce the pain associated with an inflamed nerve. The pain relief that you may experience from the injection(s) is often temporary. Typically injection(s) are administered once every 2 months for a total of 3 injections or until the pain is resolved. A sclerosing alcohol injection is placed around the involved nerve to weaken its capacity to report pain. In other words, the alcohol injection will ?deaden? the affected nerve. The pain relief that you may experience from the injection(s) can be permanent. Typically injection(s) are administered once every week for a few weeks until the pain is resolved.
Surgical Treatment
If pain persists with conservative care, surgery may be an appropriate option. The common digitial nerve is cut and the Mortons neuroma removed. This will result is numbness along the inside of the toes affected, and there is a small chance the end of the nerve will form a Stump Neuroma. Approximately 75% of people receive symptom resolution for Mortons Neuroma with conservative care.
Morton?s neuroma occurs as the nerve passes under the ligament connecting the toe bones (metatarsals) in the forefoot. Morton?s neuroma most frequently develops between the third and fourth toes, usually in response to irritation, trauma or excessive pressure. The incidence of Morton?s neuroma is 8 to 10 times greater in women than in men.Causes
Some say that this condition should not be called Morton's neuroma as, in fact, it is not actually a neuroma. A neuroma is a non-cancerous (benign) tumour that grows from the fibrous coverings of a nerve. There is no tumour formation in Morton's neuroma. The anatomy of the bones of the foot is also thought to contribute to the development of Morton's neuroma. For example, the space between the long bones (metatarsals) in the foot is narrower between the second and third, and between the third and fourth metatarsals. This means that the nerves that run between these metatarsals are more likely to be compressed and irritated. Wearing narrow shoes can make this compression worse.
Symptoms
The most common symptom of Morton's neuroma is localized pain in the interspace between the third and fourth toes. It can be sharp or dull, and is worsened by wearing shoes and by walking. Pain usually is less severe when the foot is not bearing weight.
Diagnosis
During the exam, your doctor will press on your foot to feel for a mass or tender spot. There may also be a feeling of "clicking" between the bones of your foot. Some imaging tests are more useful than others in the diagnosis of Morton's neuroma. Your doctor is likely to order X-rays of your foot, to rule out other causes of your pain such as a stress fracture. Ultrasound. This technology uses sound waves to create real-time images of internal structures. Ultrasound is particularly good at revealing soft tissue abnormalities, such as neuromas. Magnetic resonance imaging (MRI). Using radio waves and a strong magnetic field, an MRI also is good at visualizing soft tissues. But it's an expensive test and often indicates neuromas in people who have no symptoms.
Non Surgical Treatment
Depending on your overall health, symptoms and severity of the neuroma, the condition may be treated conservatively and/or with surgery. Non-surgical methods for neuroma are aimed at decreasing and/or eliminating symptoms (pain). Wear proper supportive shoes. Use an arch support. Wear shoes with a wide toe box. Modify your activities. Lose weight. Wear shoes with cushion. Prescribe an oral anti-inflammatory medication. Anti-inflammatory medication is useful to significantly reduce pain and inflammation. A physical therapist may perform ultrasound and other techniques to reduce inflammation. You will also be instructed how to stretch your foot and leg properly. Padding and/or cushioning of the ball of the foot is an effective method of preventing physical irritation with shoes. A custom foot orthotic is a doctor prescribed arch support that is made directly from a casting (mold) of your feet, and theoretically should provide superior support compared to shoe insert that you would purchase from a pharmacy. A cortisone injection is a powerful anti-inflammatory medication that is used to rapidly reduce the pain associated with an inflamed nerve. The pain relief that you may experience from the injection(s) is often temporary. Typically injection(s) are administered once every 2 months for a total of 3 injections or until the pain is resolved. A sclerosing alcohol injection is placed around the involved nerve to weaken its capacity to report pain. In other words, the alcohol injection will ?deaden? the affected nerve. The pain relief that you may experience from the injection(s) can be permanent. Typically injection(s) are administered once every week for a few weeks until the pain is resolved.
Surgical Treatment
If pain persists with conservative care, surgery may be an appropriate option. The common digitial nerve is cut and the Mortons neuroma removed. This will result is numbness along the inside of the toes affected, and there is a small chance the end of the nerve will form a Stump Neuroma. Approximately 75% of people receive symptom resolution for Mortons Neuroma with conservative care.
For Leg Length Discrepancy Chiropodists Prefer Shoe Lifts
There are not one but two unique variations of leg length discrepancies, congenital and acquired. Congenital implies that you are born with it. One leg is structurally shorter than the other. Through developmental stages of aging, the human brain picks up on the step pattern and identifies some variation. Your body typically adapts by tilting one shoulder over to the "short" side. A difference of under a quarter inch isn't blatantly abnormal, does not need Shoe Lifts to compensate and commonly does not have a serious effect over a lifetime.

Leg length inequality goes largely undiscovered on a daily basis, yet this problem is very easily remedied, and can eliminate a number of cases of back ache.
Treatment for leg length inequality typically involves Shoe Lifts. Many are cost-effective, ordinarily being under twenty dollars, in comparison to a custom orthotic of $200 if not more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Chronic back pain is the most prevalent health problem affecting people today. Around 80 million people are afflicted by back pain at some point in their life. It's a problem that costs businesses huge amounts of money annually on account of time lost and production. Innovative and more effective treatment solutions are always sought after in the hope of minimizing the economical influence this issue causes.

People from all corners of the world suffer from foot ache as a result of leg length discrepancy. In these situations Shoe Lifts can be of beneficial. The lifts are capable of eliminating any discomfort in the feet. Shoe Lifts are recommended by many professional orthopaedic physicians.
To be able to support the body in a nicely balanced manner, feet have got a significant part to play. In spite of that, it can be the most neglected area in the body. Some people have flat-feet meaning there may be unequal force exerted on the feet. This causes other areas of the body like knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
Leg length inequality goes largely undiscovered on a daily basis, yet this problem is very easily remedied, and can eliminate a number of cases of back ache.
Treatment for leg length inequality typically involves Shoe Lifts. Many are cost-effective, ordinarily being under twenty dollars, in comparison to a custom orthotic of $200 if not more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Chronic back pain is the most prevalent health problem affecting people today. Around 80 million people are afflicted by back pain at some point in their life. It's a problem that costs businesses huge amounts of money annually on account of time lost and production. Innovative and more effective treatment solutions are always sought after in the hope of minimizing the economical influence this issue causes.
People from all corners of the world suffer from foot ache as a result of leg length discrepancy. In these situations Shoe Lifts can be of beneficial. The lifts are capable of eliminating any discomfort in the feet. Shoe Lifts are recommended by many professional orthopaedic physicians.
To be able to support the body in a nicely balanced manner, feet have got a significant part to play. In spite of that, it can be the most neglected area in the body. Some people have flat-feet meaning there may be unequal force exerted on the feet. This causes other areas of the body like knees, ankles and backs to be impacted too. Shoe Lifts make sure that appropriate posture and balance are restored.
What May Cause Heel Spur

Overview
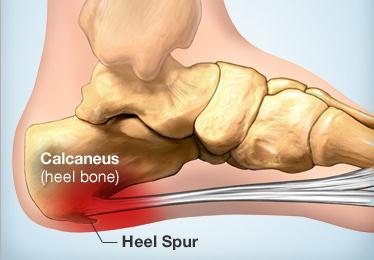
A bone spur (osteophyte) is a bony growth that forms along the edge of normal bone in response to wear and tear, most frequently in the joints. A heel spur is a bone spur of the heel bone, which causes heel pain by rubbing on the achilles tendon or other soft tissues.
Causes
Common causes of this bone spur in the heel are repetitive trauma to the base of the heel, obesity, poor walking/running technique, poorly fitting shoes, or hereditary conditions.

Symptoms
An individual with the lower legs turning inward, a condition called genu valgus or "knock knees," can have a tendency toward excessive pronation. This can lead to a fallen arch and problems with the plantar fascia and heel spurs. Women tend to suffer from this condition more than men. Heel spurs can also result from an abnormally high arch. Other factors leading to heel spurs include a sudden increase in daily activities, an increase in weight, or a thinner cushion on the bottom of the heel due to old age. A significant increase in training intensity or duration may cause inflammation of the plantar fascia. High-heeled shoes, improperly fitted shoes, and shoes that are too flexible in the middle of the arch or bend before the toe joints will cause problems with the plantar fascia and possibly lead to heel spurs.
Diagnosis
Diagnosis is made using a few different technologies. X-rays are often used first to ensure there is no fracture or tumor in the region. Then ultrasound is used to check the fascia itself to make sure there is no tear and check the level of scar tissue and damage. Neurosensory testing, a non-painful nerve test, can be used to make sure there is not a local nerve problem if the pain is thought to be nerve related. It is important to remember that one can have a very large heel spur and no plantar fasciitis issues or pain at all, or one can have a great deal of pain and virtually no spur at all.
Non Surgical Treatment
There are many temporary solutions to resolve the pain associated with irritation to the plantar ligaments. Common recommendations are ice and anti-inflammatory medications or even cortisone injections, however none of these solve the fundamental problem. To permanently resolve heel spurs you need to support and restrict the movement of the plantar ligaments. Flexible shoes will aggravate and often contribute to heel spurs. We recommend a RIGID orthotic that extends from the metatarsal heads to the heel to resolve heel spurs.
Surgical Treatment
Have surgery if no other treatments work. Before performing surgery, doctors usually give home treatments and improved footwear about a year to work. When nothing else eases the pain, here's what you need to know about surgical options. Instep plantar fasciotomy. Doctors remove part of the plantar fascia to ease pressure on the nerves in your foot. Endoscopy. This surgery performs the same function as an instep plantar fasciotomy but uses smaller incisions so that you'll heal faster. However, endoscopy has a higher rate of nerve damage, so consider this before you opt for this option. Be prepared to wear a below-the-knee walking cast to ease the pain of surgery and to speed the healing process. These casts, or "boots," usually work better than crutches to speed up your recovery time.
Prevention
To prevent this condition, wearing shoes with proper arches and support is very important. Proper stretching is always a necessity, especially when there is an increase in activities or a change in running technique. It is not recommended to attempt working through the pain, as this can change a mild case of heel spurs and plantar fascitis into a long lasting and painful episode of this condition.
What Is The Most Suitable Answer To Heel Spur

Overview
Heel spur is a hook of bone that protrudes from the bottom of the foot where plantar fascia connects to the heel bone. Pain associated with heel spurs is usually pain from plantar fasciitis, not the actual bone. Heel spurs are most often diagnosed when a patient has visited a pain specialist or podiatrist for on-going foot pain related to plantar fasciitis; spurs are diagnosed via X-ray of the foot. Heel spurs are most commonly diagnosed in middle-aged men and women. As noted, most patients with this condition have other podiatry-related pain. This condition is a result of plantar fasciitis (when the fascia, a thick connective tissue that connects the heel bone and ball of the foot) becomes inflamed. Some 70% of plantar fasciitis patients have a bone spur. Bone spurs are soft calcium deposits caused from tension in the plantar fascia. When found on an X-ray, they are used as evidence that a patient is suffering from plantar fasciitis. Plantar fasciitis is typically caused from repetitive stress disorder. Walking, running, and dancing can cause this with time.
Causes
Though this syndrome is most common in individuals 40 years or older, it can occur at any age. The following factors increase the likelihood of heel spur development. An uneven gait which applies too much pressure to certain areas of the foot. Being overweight. Wearing worn shoes or ill-fitting footwear. Job conditions that require long periods spent standing or lifting heavy objects. The normal aging process which results in a decrease in ligament elasticity.

Symptoms
Heel spur is characterised by a sharp pain under the heel when getting out of bed in the morning or getting up after sitting for a period of time. Walking around for a while often helps reduce the pain, turning it into a dull ache. However, sports, running or walking long distance makes the condition worse. In some cases swelling around the heel maybe present.
Diagnosis
Your doctor, when diagnosing and treating this condition will need an x-ray and sometimes a gait analysis to ascertain the exact cause of this condition. If you have pain in the bottom of your foot and you do not have diabetes or a vascular problem, some of the over-the-counter anti-inflammatory products such as Advil or Ibuprofin are helpful in eradicating the pain. Pain creams, such as Neuro-eze, BioFreeze & Boswella Cream can help to relieve pain and help increase circulation.
Non Surgical Treatment
Rest your foot. Reduce the amount of weight-bearing activities you participate in. Get off of your feet and elevate them. This will allow healing to begin. Apply ice to your foot. Applications of ice packs that provide a comfortable cooling to the heel and arch (not a freezing cold) will help reduce pain, swelling, and inflammation. Apply the ice to the heel and arch (not the toes). Make sure it is comfortable, and leave on your foot for about 20 minutes, 3 times a day. If you have any medical problems such as diabetes, poor circulation, etc., discuss the use of ice with your doctor before applying the ice. Active Wrap allows you to apply comfortable cold therapy to your foot without messy ice cubes. Use while on the ?go.? Do not walk with bare feet. Always protect your heels, arches, and plantar fascia with good supportive shoes. Vionic Orthotic Flip Flops For Men and Women are designed for walking comfort with built in orthotic foot beds that help reduce foot pain from heel spurs. Use in the house or on the beach.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.
Prevention
Prevention of heel spur syndrome may be best by finding a good supportive shoe. Never go barefoot or wear a flat soled shoe. There are many over the counter arch supports that give increased support for your feet. Usually when there is excessive pronation the Achilles Tendon contracts or becomes shortened over time since it is not being used fully. The shortened Achilles Tendon is called an equinus deformity. By keeping this tendon stretched it may decrease some of the tension in the foot. Some theories believe the Achilles Tendon and plantar fascia is continuous. Before you get up from rest, stretch out your Achilles and the plantar fascia. You may attempt to spell the alphabet with your foot and ankle, use a towel against pressure on your foot, or roll a can of soup or sodapop on the ground. Ice may work well at the times of severe pain. For a chronic pain, or longer lasting pain heat therapy may improve the condition.